Porto-sinusoidal Vascular Disease: 영상의학과 의사가 알아야 할 것
Porto-sinusoidal Vascular Disease: What Radiologists Should Know
Article information

Abstract
Porto-sinusoidal vascular disease (PSVD)는 문맥고혈압을 유발할 수 있는 비교적 드문 간의 혈관질환이다. PSVD는 간경화와 유사한 임상소견을 보이기 때문에 임상적으로는 진단이 어렵다. 하지만 영상의학적 검사는 PSVD와 간경화의 감별에 중요한 단서를 제공할 수 있다. 이 종설은 단면영상 및 초음파탄성측정법에서 PSVD를 시사하는 소견에 대해 알아보고, 이를 통해 임상의에게 PSVD의 진단에 필수적인 조직검사를 제안할 수 있게 한다.
Trans Abstract
Porto-sinusoidal vascular disease (PSVD) is a rare hepatic vascular disorder that can cause portal hypertension. Its diagnosis can be challenging, as its clinical manifestations can overlap with those of liver cirrhosis. However, radiological imaging can provide valuable clues to differentiate PSVD from liver cirrhosis. This review aims to identify imaging findings that suggest PSVD in cross-sectional imaging and ultrasound elastography, enabling the suggestion of a liver biopsy that is essential for diagnosis of PSVD.
서 론
문맥고혈압은 주로 간경화와 같은 진행된 만성간질환 (advanced chronic liver disease) 환자에서 발생하며, 정맥류 출혈, 복수, 간성혼수 등의 다양한 합병증을 일으킬 수 있다[1]. 이는 주로 만성 바이러스간염, 과다 알코올 섭취, 비만 또는 기타 대사 이상으로 인한 진행된 만성간질환 환자에서 발생한다. 하지만, 순간탄성측정법 (transient elastography) 같은 비침습적인 검사가 많이 시행되면서 간탄성도 (liver stiffness) 측정치가 높지 않아도 문맥고혈압이 있거나, 문맥고혈압이 간 섬유화 정도와 일치하지 않는 경우가 종종 발견되었고 이를 idiopathic portal hypertension, non-cirrhotic portal fibrosis, hepatoportal sclerosis 등의 다양한 명칭으로 혼용하여 사용하였다[2].
이에 2016년 유럽간학회에서는 Schouten 등의 연구를 참고하여 간경화가 없는 문맥고혈압 환자 중에서 문맥고혈압의 원인이 불분명하고 간문맥이나 간정맥 폐쇄가 없는 경우를 통칭하여 idiopathic noncirrhotic portal hypertension (INCPH)으로 정의하였다[2, 3]. 하지만 이 정의는 몇가지 제한점이 있는데, INCPH의 초기에는 문맥고혈압이 발현되지 않을 수 있고, 바이러스간염이나 알코올성 간질환이 INCPH 환자에게 동반될 수 있으며, 약 40%의 INCPH 환자에서 경과 중에 간문맥혈전이 발생한다는 것이 알려졌기 때문이다[4].
이러한 제한점을 극복하기 위해 2019년 Vascular Liver Disease Interest Group은 새로운 개념을 제안하였고, 대부분의 병변이 intrahepatic portal venule이나 sinusoid를 침범하여 대부분 sinusoid 전단계의 문맥고혈압 (presinusoidal portal hypertension)을 유발하기에 이를 porto-sinusoidal vascular disease (PSVD)로 명명하였다[4]. 따라서 PSVD는 INCPH 보다 질환의 다양한 측면을 반영하는 좀 더 포괄적인 개념이다.
정의 및 진단기준
PSVD의 정의는 조직학적으로 간경화가 없고, 문맥고혈압의 여부와는 상관없이 이 질환을 시사하는 임상적인 징후나 조직학적 병변이 있는 경우를 기반으로 한다[4]. 따라서 간 조직검사가 진단에 필수적이다. 이에 더해 1) 문맥고혈압을 시사하는 한 개 이상의 특이적인 임상 징후가 있거나, 2) PSVD를 시사하는 한 개 이상의 특이적인 조직학적 병변이 있거나, 3) 한 개 이상의 비특이적인 임상적 징후와 조직학적 병변이 함께 있는 경우 진단할 수 있다 (Table 1). 정의상으로는 간경화가 없는 환자에서 문맥고혈압을 시사하는 특이적인 임상적 징후가 없더라도 obliterative portal venopathy, nodular regenerative hyperplasia, incomplete septal fibrosis/cirrhosis와 같은 특이적인 조직학적 병변이 있다면 PSVD를 진단할 수 있다. 하지만 Budd-Chiari syndrome, sinusoidal obstruction syndrome과 같은 간정맥유출로 폐쇄와 연관된 질환이나 미세혈관손상과 연관있는 sarcoidosis, congenital hepatic fibrosis 등의 질환은 PSVD에서 제외된다[4].
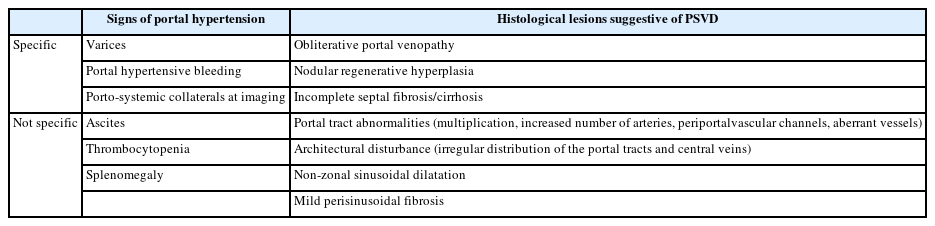
Definition and diagnostic criteria of porto-sinusoidal vascular disease
PSVD와의 관련성이 제기된 여러 약제나 간외질환들이 알려져 있는데, 면역질환이나 혈액질환을 치료하기 위해 사용하는 일부 면역억제제와 질환 그 자체, HIV의 치료제와 HIV 감염 그 자체, 그리고 혈전유발상태 (prothrombotic condition) 등이 있다 (Table 2) [4].
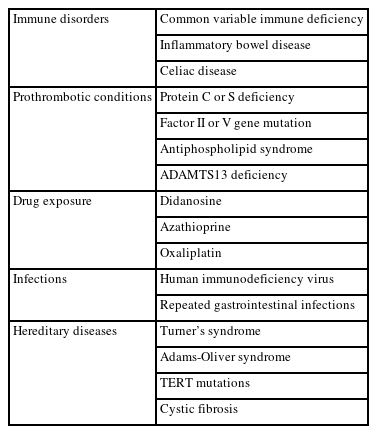
Extrahepatic conditions known to be associated with portosinusoidal vascular disease
임상적인 측면
문맥고혈압이 동반된 PSVD 환자들의 가장 흔한 이상 검사소견은 저혈소판증이다[4]. 80% 이상의 환자에서 경미한 간수치의 증가가 있다[5]. 문맥고혈압의 합병증으로 20-44%의 환자에서 초기 진단시 정맥류 출혈을 보이며, 약 20-50%의 환자에서 복수가 발생한다[6, 7]. 또한 PSVD의 진단 후 5년 이내에 약 30-40%에서 간문맥 혈전증이 발생한다는 보고도 있다[6-8]. 하지만 이런 징후는 간경화에서도 동일하게 나타날 수 있기 때문에 임상적으로 문맥고혈압이 동반된 PSVD를 간경화로 오인할 수 있고 최종 진단이 지연될 가능성이 있다. 한 연구에 따르면, PSVD 환자의 약 72%가 처음에 간경화로 오인되었고, PSVD로 최종 진단되기까지의 중위 시간은 32개월이었다[9]. PSVD와 간경화 모두 문맥고혈압에 동반될 수 있는 합병증들을 예방하고 합병증이 발생한 경우 그에 맞는 치료를 해야한다는 점에서 동일하지만, PSVD는 간경화보다 상대적으로 간기능이 더 보존되어 있고 예후도 더 좋은 것으로 알려져 있어 차이점이 존재한다[10]. 또한 만성 바이러스간염이나 알코올성 간질환이 동반되지 않은 PSVD의 경우 간암 (hepatocellular carcinoma) 발생 감시 (surveillance)의 필요성이 높지 않기 때문에 간경화와의 감별이 중요하다[4]. 하지만 임상적으로는 두 개의 질환을 구분하는 것이 쉽지 않기 때문에 문맥고혈압이 있는 경우 평가를 위해 시행하는 초음파, CT, MRI, 초음파탄성측정법 (ultrasound elastography)과 같은 검사를 통해 PSVD의 가능성을 제시할 수 있어야 하겠다. 이를 통해 필요시 PSVD의 진단을 위해 필수적인 간 조직검사를 임상의에게 제안하는 것이 영상의학과 의사의 역할이라고 할 수 있겠다.
영상의학적 소견
여러 연구들에 따르면 간경화와 비교하여 PSVD를 시사하는 영상의학적 소견들이 보고가 되었다 (Table 3). CT나 MRI와 같은 단면영상에서 가장 중요한 감별점은 간경화의 전형적인 소견인 간표면결절성 (liver surface nodularity)이 PSVD에서는 낮은 비율로 보인다는 점이다 (Fig. 1A). 한 연구에 따르면 정성적으로 판단한 간표면결절성의 비율이 간경화에서는 약 89% 였으나, PSVD에서는 약 16% 였다[9]. 간표면결절성을 정량적으로 측정하는 반자동 프로그램을 사용한 연구에서도 이와 동일한 결과를 보였다[11]. 미상엽의 비대는 간경화와 PSVD에서 의미있는 차이를 보이지 않았으나 4구역의 위축 소견은 PSVD보다 간경화에서 흔하게 관찰되었고, 4구역의 너비는 그 자체로도 PSVD와 간경화를 감별하는데 도움을 주는 소견이지만 간표면결절성의 여부와 함께 고려시 두 질환의 감별에 대한 진단능이 좀 더 향상되는 것으로 보고되었다 (Fig. 1E) [9, 11-13]. 이와 함께 문맥고혈압이 동반된 PSVD와 간경화 모두 정맥류나 복수, 비장비대가 보일 수 있지만, 비슷한 간기능을 보이는 경우 문맥고혈압의 정도는 간경화보다 PSVD가 좀 더 심한 경향을 보였다[9].
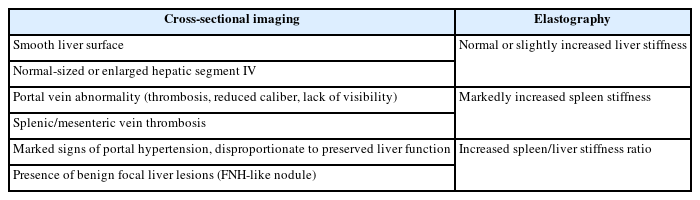
Imaging findings suggestive of porto-sinusoidal vascular disease rather than liver cirrhosis

A 44-year-old man with porto-sinusoidal vascular disease diagnosed by percutaneous liver biopsy.
A–B. CT shows smooth liver surface (arrow in A) and findings of portal hypertension shown as splenomegaly and gastric varix (arrowhead in A). Note that the portal vein (arrow in B) and splenic vein (arrowheads in B) are patent. Histological finding of the biopsy specimen (not shown on the figure) shows a complete absence of the portal vein (obliterative portal venopathy). C–D. Ultrasound elastography using 2D shear wave elastography shows mild increase in liver stiffness (median liver stiffness value, 6.4 kPa shown on C), whereas spleen stiffness is markedly increased (median spleen stiffness value, 46.1 kPa shown on D). E–F. After 11 years, CT on the same patient shows that the overall volume of the liver has decreased, while the volume of segment IV has been preserved (arrowheads in E). Also, note that thrombosis has developed in the main portal vein (arrow in E) and splenic vein (arrows in F).
조영증강 CT나 MRI에서 보이는 간문맥 이상 여부가 두 질환의 감별에 도움을 줄 수 있다. PSVD는 진단기준에서도 알 수 있듯이 obliterative portal venopathy가 주요 조직학적 병변이기 때문에 간경화보다 간문맥 이상 소견이 더 자주 발견된다 (Figs. 1E and 1F). 한 연구에 따르면 간내 및 간외문맥의 이상 소견 (혈전증, 문맥 직경의 감소, 간내문맥의 숫자 감소)의 비율이 간경화에서는 17%, PSVD에서는 71% 였다[14]. 다른 연구에서는 조영증강 CT의 동맥기나 문맥기에서 간실질의 비균질 조영증강 (heterogenous enhancement)의 비율이 간경화보다 PSVD에서 높았고, 간세포특이조영제를 사용한 MRI에서는 비슷한 간기능을 보이는 경우 간담도기 (hepatobiliary phase)에서 간실질의 신호강도가 주변 혈관에 비해서 높은 경우가 간경화보다 PSVD에서 더 자주 보인다고 보고하였다[9, 13].
초음파탄성측정법도 두 질환의 감별에 도움을 줄 수 있다. 일반적으로 간경화보다 PSVD에서 간탄성도가 낮게 측정되며 PSVD 환자에서 보고된 간탄성도의 중앙값은 6.2-8.4 kPa이다 (Fig. 1C) [15-17]. 순간탄성측정법을 이용한 한 연구에 의하면 Baveno VI consensus에서 차용한 10 kPa과 20 kPa을 각각 PSVD의 진단 및 제외 기준으로 삼았을 경우 PSVD와 간경화의 감별을 위한 진단능은 민감도 94%, 특이도 96% 이상으로 보고하였다[1]. 중간지대 (gray zone) 인 10-20 kPa의 환자의 경우 간경화의 뚜렷한 원인이 없거나 PSVD와 연관된 간외질환이 있는 경우 PSVD의 가능성을 배제할 수 없으므로 간조직검사를 고려해야 한다고 주장하였다[18]. 또 다른 연구에 의하면 비장탄성도 (spleen stiffness) 측정시 그 정도는 간경화보다 PSVD에서 유의하게 높았다 (Fig. 1D) [16, 17]. 따라서 문맥고혈압이 있는 환자에서 간탄성도의 수치가 정상이거나 약간 높고 비장탄성도의 수치가 높은 경우 PSVD의 가능성을 고려해야 하겠다[16, 19].
PSVD에서 가장 흔한 국소간병변은 양성 병변인 국소결절증식양 결절 (focal nodular hyperplasia-like nodule)이며 약 12.5-14.0%에서 발견된다[9, 20]. 간암과의 영상의학적 감별이 중요한데 두 질환 모두 동맥기에서 강한 조영증강을 보이나 간암과는 달리 국소결절증식양 결절은 문맥기 혹은 지연기 씻김 (washout)이 없고 간세포특이조영제를 사용한 MRI에서 간담도기에 주변 간조직과 비슷하거나 높은 신호강도를 보이는 것이 특징적이다. 정의 및 진단 기준 참고시 PSVD에서 간암의 위험인자인 만성간질환이 동반될 수 있기 때문에 동반된 만성 간질환의 비율에 따라 간암의 발생률이 다양하게 보고되었다. 동반된 만성간질환이 없는 43명의 PSVD 환자로 구성된 한 연구에서는 중위 46개월의 추적관찰동안 간암이 발생하지 않았으나[9], 다른 연구에서는 91명의 PSVD 환자 중 30% 이상의 환자에서 만성간질환이 있었고 중위 37개월의 추적관찰동안 2명의 환자에서 간암이 발생하였다[21].
문맥고혈압 환자에서 조직검사가 필요한 경우
이와 같은 영상의학적 소견들을 종합하여 문맥고혈압의 징후가 있는 환자에서 원인 질환을 감별하기 위해 조직검사가 필요한 경우를 알아보고자 한다 (Fig. 2). CT나 MRI와 같은 단면영상에서는 간표면결절성 및 4구역위축 여부를 각각 평가기준으로 삼아 판단하며[11], 초음파탄성측정법에서는 순간탄성측정법을 기준으로 Baveno VI consensus에서 차용한 10 kPa과 20 kPa의 두개의 절단 값 (dual cut-off)을 사용한다[1, 18]. 간표면결절성과 4구 역위축이 모두 있는 경우와 간탄성도가 20 kPa 이상인 경우 PSVD보다는 간경화의 가능성이 높고, 그 외의 경우는 PSVD의 가능성을 배제할 수 없기 때문에 필요시 간 조직 검사를 고려해야 한다. 단면영상과 초음파탄성측정법 모두 두개의 평가기준과 두개의 절단값을 사용하므로 중간지대가 발생한다. 즉 단면영상에서는 간표면이 매끈하거나 4구역의 크기가 정상이거나 약간 증가한 경우, 초음파탄성측정법에서는 간탄성도가 10-20 kPa인 경우이며, 특히 환자가 간경화의 뚜렷한 원인이 없거나 PSVD와 연관된 간외질환이 있는 경우 PSVD의 가능성을 배제할 수 없으므로 간조직검사를 고려해야 한다.

Cases of portal hypertension where liver biopsy should be considered on cross-sectional imaging and transient elastography.
LSM = liver stiffness measurement; PSVD = porto-sinusoidal vascular disease.
결 론
Porto-sinusoidal vascular disease는 idiopathic noncirrhotic portal hypertension의 엄격한 정의에서 제기된 제한점들을 극복하기 위해 비교적 최근에 제안된 개념으로 아직 의사들에게 잘 알려져 있지 않은 질환이다. 문맥고혈압과 연관된 징후로 발현하는 경우가 많기 때문에 임상적으로는 간경화와 구분이 쉽지 않으나 영상 검사를 통해 두 질환의 감별에 도움을 주는 단서를 얻을 수 있다. 따라서 영상의학과 의사는 문맥고혈압의 평가를 위해 시행한 영상 검사에서 간경화와 구분되는 PSVD의 소견에 대해 알고 있어야 하며 PSVD의 진단을 위해 필수적인 조직검사를 제안할 수 있어야 하겠다.
Notes
Funding
The authors state that this work has not received any funding.
Conflict of Interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.